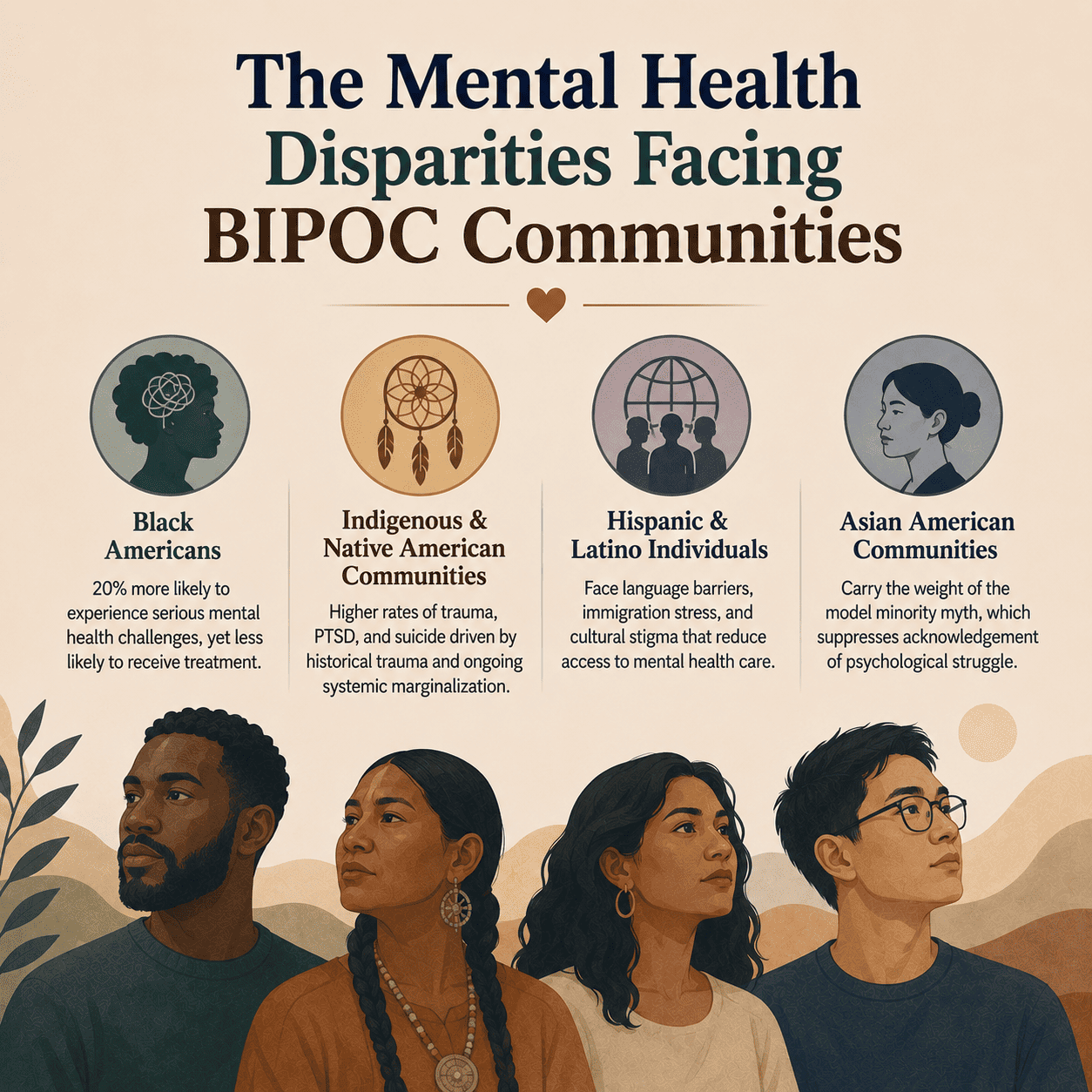
Black Americans are 20 percent more likely to experience serious mental health challenges than the general population, yet significantly less likely to receive treatment.
Indigenous and Native American communities experience rates of trauma, PTSD, and suicide that far exceed national averages, driven by the compounding effects of historical trauma, land displacement, and ongoing systemic marginalization. Hispanic and Latino individuals often face language barriers, immigration-related stress, and cultural stigma that dramatically reduce mental health help-seeking. Asian American communities carry the weight of the model minority myth – a cultural expectation of silent resilience that actively suppresses acknowledgment of psychological struggle.
These are not coincidences. They are the predictable outcomes of systems that were not designed with BIPOC communities in mind – and in many cases were designed to actively work against them.